КАТЕГОРИИ:
Архитектура-(3434)Астрономия-(809)Биология-(7483)Биотехнологии-(1457)Военное дело-(14632)Высокие технологии-(1363)География-(913)Геология-(1438)Государство-(451)Демография-(1065)Дом-(47672)Журналистика и СМИ-(912)Изобретательство-(14524)Иностранные языки-(4268)Информатика-(17799)Искусство-(1338)История-(13644)Компьютеры-(11121)Косметика-(55)Кулинария-(373)Культура-(8427)Лингвистика-(374)Литература-(1642)Маркетинг-(23702)Математика-(16968)Машиностроение-(1700)Медицина-(12668)Менеджмент-(24684)Механика-(15423)Науковедение-(506)Образование-(11852)Охрана труда-(3308)Педагогика-(5571)Полиграфия-(1312)Политика-(7869)Право-(5454)Приборостроение-(1369)Программирование-(2801)Производство-(97182)Промышленность-(8706)Психология-(18388)Религия-(3217)Связь-(10668)Сельское хозяйство-(299)Социология-(6455)Спорт-(42831)Строительство-(4793)Торговля-(5050)Транспорт-(2929)Туризм-(1568)Физика-(3942)Философия-(17015)Финансы-(26596)Химия-(22929)Экология-(12095)Экономика-(9961)Электроника-(8441)Электротехника-(4623)Энергетика-(12629)Юриспруденция-(1492)Ядерная техника-(1748)
Testicular Torsion
|
|
|
|
Torsion of the testicle results from twisting of the spermatic cord, which compromises testicular blood supply. The number of twists determines the amount of vascular impairment, although generally a 4- to 8-hour window exists before significant ischemic damage occurs that can affect long-term testicular morphology and sperm formation. Testicular torsion is a true surgical emergency. Adolescent males tend to present beyond the “golden” 4- to 8-hour period, but urgent surgical treatment is indicated because viability of the testis is difficult to predict.
Testicular torsion is commonly observed in males younger than 30 years, with a peak at 12-18 years. The incidence of torsion in males younger than 25 years is approximately 1 in 4000. Torsion more often involves the left testicle. The etiologic factors involved in intravaginal testicular torsion include congenital anomaly, bell clapper deformity, undescended testicle, sexual arousal or activity, exercise, active cremasteric reflex, and cold weather.
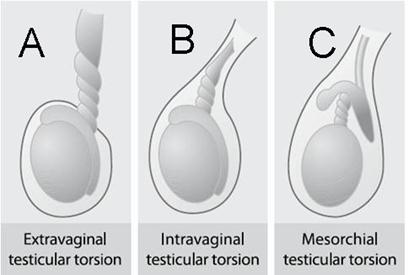
| The types of testicular torsion: |
|
Testicular torsion is a lesion that presents by one of two mechanisms. In newborns, torsion occurs external to the tunica vaginalis because the tunica vaginalis is only weakly attached to the overlying dartos muscle (A). After 6 to 8 weeks of extrauterine life, these attachments become much stronger and extravaginal torsion is exceedingly uncommon. Torsion of the cord in an older child occurs because there is a lack of the normal attachments between the epididymis and the tunica vaginalis or because the mesorchium is somewhat longer than normal (B and C).
* Extravaginal torsion results from twisting of the cord proximal to the tunica vaginalis. This mechanism occurs perinatally during descent of the testicle before the scrotal investment of the tunica vaginalis has taken place, allowing the tunica and testis to spin on their vascular pedicles. The tunica vaginalis likely becomes adherent to the surrounding tissues by 6 weeks of age.
* Intravaginal torsion occurs beyond the perinatal period and can result from abnormal fixation of the testicle and epididymis within the tunica vaginalis. Normally, the tunica invests the epididymis and posterior surface of the testicle, which fixes it to the scrotum and prevents it from twisting. If the tunica vaginalis attaches in a more proximal position on the spermatic cord, the testicle and epididymis hang free in the scrotum and can twist within the tunica vaginalis. Such abnormal fixation is described classically as the “bell-clapper” deformity and occurs in only a minority of males (Image 8.1). This type of deformity is common, as discerned by autopsy studies, and usually is bilateral. Because testicular torsion occurs relatively infrequently, other factors also play a role in its occurrence.
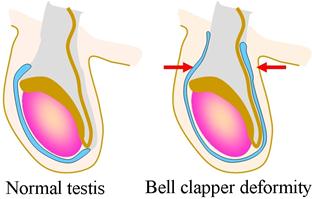 Image 8.1 Bell clapper deformity, a congenital condition in which the testis hangs within the scrotum (red arrows) and can swing like a bell clapper in a bell, allowing for easy torsion. Males born with the bell clapper deformity have no attachments around either testicle, so that torsion can potentially occur on either side. The bell clapper deformity is present in approximately 12% of males; 40% of them are affected in both testicles.Bilateral testicular torsion, however, is an exceedingly rare event. Image 8.1 Bell clapper deformity, a congenital condition in which the testis hangs within the scrotum (red arrows) and can swing like a bell clapper in a bell, allowing for easy torsion. Males born with the bell clapper deformity have no attachments around either testicle, so that torsion can potentially occur on either side. The bell clapper deformity is present in approximately 12% of males; 40% of them are affected in both testicles.Bilateral testicular torsion, however, is an exceedingly rare event.
|
Rapid growth and increasing vascularity of the testicle also may be precursors to torsion. This phenomenon occurs at puberty and is believed to account for the age distribution of torsion, which increases in adolescence. Rapid cremasteric muscle contraction elevates the testicle and can have a rotational effect on the spermatic cord that can induce torsion. The congestion associated with an inflammatory process or minor trauma also may predispose to torsion in a male who has a “bell-clapper” deformity. It is especially important to maintain a high level of suspicion in boys who experience increasing pain after being diagnosed as having epididymitis or mild blunt scrotal trauma, who may have developed testicular torsion as a secondary event.
|
|
|
|
|
Дата добавления: 2014-10-15; Просмотров: 4926; Нарушение авторских прав?; Мы поможем в написании вашей работы!