КАТЕГОРИИ:
Архитектура-(3434)Астрономия-(809)Биология-(7483)Биотехнологии-(1457)Военное дело-(14632)Высокие технологии-(1363)География-(913)Геология-(1438)Государство-(451)Демография-(1065)Дом-(47672)Журналистика и СМИ-(912)Изобретательство-(14524)Иностранные языки-(4268)Информатика-(17799)Искусство-(1338)История-(13644)Компьютеры-(11121)Косметика-(55)Кулинария-(373)Культура-(8427)Лингвистика-(374)Литература-(1642)Маркетинг-(23702)Математика-(16968)Машиностроение-(1700)Медицина-(12668)Менеджмент-(24684)Механика-(15423)Науковедение-(506)Образование-(11852)Охрана труда-(3308)Педагогика-(5571)Полиграфия-(1312)Политика-(7869)Право-(5454)Приборостроение-(1369)Программирование-(2801)Производство-(97182)Промышленность-(8706)Психология-(18388)Религия-(3217)Связь-(10668)Сельское хозяйство-(299)Социология-(6455)Спорт-(42831)Строительство-(4793)Торговля-(5050)Транспорт-(2929)Туризм-(1568)Физика-(3942)Философия-(17015)Финансы-(26596)Химия-(22929)Экология-(12095)Экономика-(9961)Электроника-(8441)Электротехника-(4623)Энергетика-(12629)Юриспруденция-(1492)Ядерная техника-(1748)
Embolectomy via the Brachial Artery
Embolectomy
Operation
As mentioned previously, the most common site for embolic obstruction is the brachial artery.
The arm is placed on an arm table. We prefer to perform embolectomy using local anesthesia. Often a transverse incision placed over the palpable brachial pulse can be used. If proximal extension of the incision is required, this should be done in parallel with and dorsal to the dorsal aspect of the biceps muscle. It has to be kept in mind that 10–20% of patients may have a different brachial artery anatomy. The most common variation is a high bifurcation of the radial and ulnar arteries, and next in frequency is a doubled brachial artery.
An alternative location for embolectomy in the arm is to expose the brachial artery in the bicipital groove. A longitudinal incision starting 10 cm above the elbow that is extended proximally is then used.
If it is hard to achieve a good inflow, a proximal lesion may cause the embolization or thrombosis. More complicated vascular procedures are then required to reestablish flow. The embolectomy attempt is then discontinued and the patient taken to the angiography suite for a complete examination. If practically feasible, an alternative is to obtain the angiogram in the operating room. Frequently, however, the preferred treatment is endovascular, and this is better done in the angiography suite. Occasionally the films will reveal a proximal obstruction that needs open repair. Examples of such are carotid-subclavian, subclavian-axillary, and axillary-brachial bypasses.
Brachial Artery in the Upper Arm
The incision is made along the posterior border of the biceps muscle; a length of 6–8 cm is usually enough.
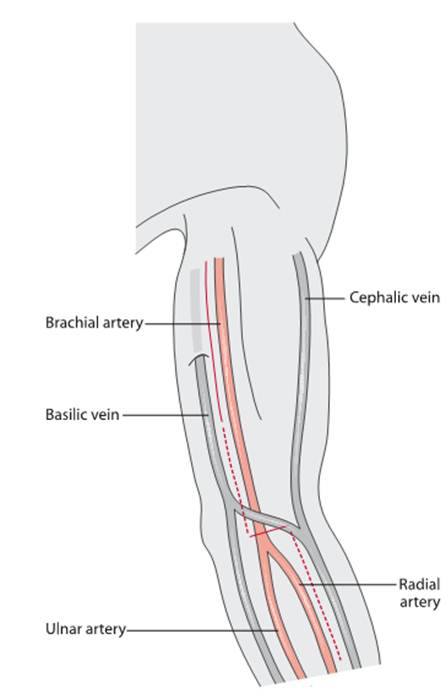
Fig. Transverse incision in the elbow for exposing the brachial artery and with possible elongations (dottedlines) when access to the ulnar and radial branches as well as to more proximal parts of the brachial artery is needed
The muscles are retracted medially and laterally, and the artery lies in the neurovascular bundle immediately below the muscles. The sheath is incised and the artery freed from the median nerve and the medial cutaneous nerve that surrounds it.
Brachial Artery at the Elbow
The incision is placed 2 cm below the elbow crease and should continue up on the medial side along the artery. If possible, veins transversing the wound should be preserved, but they can be divided if necessary for exposure. The medial insertion of the biceps tendon is divided entirely, and the artery lies immediately beneath it. By following the wound proximally, more of the artery can be exposed. If the origins of the radial and ulnar artery need to be assessed, the wound can be elongated distally on the ulnar side of the volar aspect of the arm. The median nerve lies close to the brachial artery, and it is important to avoid injuring it.
A transverse arteriotomy in the brachial artery is made as close as possible to the bifurcation of the ulnar and radial arteries. The embolectomy is performed in proximal and distal directions with #2 and #3 Fogarty catheters. Separate embolectomy in each branch should be done if technically simple. The Fogarty catheter otherwise slips down into the larger and straighter ulnar artery. The route of the catheter can be checked by palpation at the wrist level when the inflated balloon passes. On the other hand, restored flow in one of the arteries is usually enough for a result that is sufficient for adequate hand perfusion. The arteriotomy is closed with interrupted 6-0 sutures, and distal pulses and the perfusion in the hand are evaluated. If the result is inadequate – poor backflow after embolectomy, absence of pulse, a weak continuous-wave Doppler signal, and questionable hand perfusion – the arteriotomy should be reopened and intraoperative angiography performed.
|
|
Дата добавления: 2014-12-23; Просмотров: 1012; Нарушение авторских прав?; Мы поможем в написании вашей работы!