КАТЕГОРИИ:
Архитектура-(3434)Астрономия-(809)Биология-(7483)Биотехнологии-(1457)Военное дело-(14632)Высокие технологии-(1363)География-(913)Геология-(1438)Государство-(451)Демография-(1065)Дом-(47672)Журналистика и СМИ-(912)Изобретательство-(14524)Иностранные языки-(4268)Информатика-(17799)Искусство-(1338)История-(13644)Компьютеры-(11121)Косметика-(55)Кулинария-(373)Культура-(8427)Лингвистика-(374)Литература-(1642)Маркетинг-(23702)Математика-(16968)Машиностроение-(1700)Медицина-(12668)Менеджмент-(24684)Механика-(15423)Науковедение-(506)Образование-(11852)Охрана труда-(3308)Педагогика-(5571)Полиграфия-(1312)Политика-(7869)Право-(5454)Приборостроение-(1369)Программирование-(2801)Производство-(97182)Промышленность-(8706)Психология-(18388)Религия-(3217)Связь-(10668)Сельское хозяйство-(299)Социология-(6455)Спорт-(42831)Строительство-(4793)Торговля-(5050)Транспорт-(2929)Туризм-(1568)Физика-(3942)Философия-(17015)Финансы-(26596)Химия-(22929)Экология-(12095)Экономика-(9961)Электроника-(8441)Электротехника-(4623)Энергетика-(12629)Юриспруденция-(1492)Ядерная техника-(1748)
Acute upper extremity ischemia
|
|
|
|
TOPIC 9. ARTERIAL TROMBOSIS AND EMBOLISM
О САМОСТОЯТЕЛЬНОМ ХАРАКТЕРЕ ПИСЬМЕННОЙ РАБОТЫ
ЗАЯВЛЕНИЕ
Степанову С.С.
Ректору
НОУ ВПО «Академия МНЭПУ»
Я, ____________________________________________________________,
(ФИО полностью)
студент (слушатель) _____ курса _________________________ формы обучения
(очной, очно-заочной, заочной)
специальности (направления) ___________________________________________
(Наименование специальности (направления))
____________________________________________________________________
заявляю, что в моей письменной работе __________________________________
(Указать вид письменной работы)
на тему «__________________________________________________________»,
(Название работы)
представленной на кафедру или в государственную аттестационную комиссию для публичной защиты, не содержится элементов плагиата.
Все прямые заимствования из печатных и электронных источников, а также из защищенных ранее письменных работ, кандидатских и докторских диссертаций имеют соответствующие ссылки.
Я ознакомлен(а) с действующим в Академии «Положением об использовании системы «Антиплагиат» в учебной и научной деятельности», согласно которому обнаружение плагиата является основанием для выставления отрицательной оценки или недопуска письменной работы к защите.
_______________________ (______________________)
(Подпись и расшифровка подписи обучающегося
«___» _________________ 20 __ г.
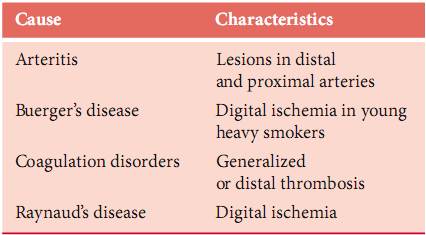
Acute ischemia in the upper extremity constitutes 10–15% of all acute extremity ischemia. The etiology is emboli in 90% of the patients. The reason for this higher rate compared with the leg is that atherosclerosis is less common in arm arteries. Emboli have the same origins as in the lower extremity and usually end up obstructing the brachial artery. Sometimes plaques or an aneurysm in the subclavian or axillary arteries is the primary source of emboli. Embolization to the right arm is more common than to the left due to the vascular anatomy. For the 10% of patients with atherosclerosis and acute thrombosis as the main cause for their arm ischemia, the primary lesions are located in the brachiocephalic trunk or in the subclavian artery. Such pathologies are usually asymptomatic due to well-developed collaterals around the shoulder joint until thrombosis occurs, and they cause either micro- or macroembolization. Other less frequent causes of acute upper extremity ischemia are listed in Table 1
Table 1. Less common causes of acute upper extremity ischemia
Subclavian artery thrombosis is a condition in which the blood flow through the vessel is obstructed. The condition usually occurs secondary to some form of antecedent injury to the vessel, hypercoagulable state, or atherosclerotic changes. The condition is common in young athletic individuals who exert a significant amount of upper body activity. Sudden occlusion from emboli followed by thrombosis of the artery is common in the population with signs of significant atherosclerotic disease.
The patient presenting with acute subclavian artery occlusion usually has a history of repetitive use and/or stress injury to the upper extremity on the affected side. A history of upper extremity claudication is common.
In situations in which the occlusion is secondary to atherosclerosis, acute thromboses of the artery are generally asymptomatic. In fact, in 9% of autopsy series, the left subclavian artery was either stenotic or occluded. If symptoms are present, upper extremity claudication on the affected side is most common. The patient may also present with dizziness, vertigo, imbalance, visual disturbances, or hemisensory dysfunction indicative of a subclavian steal syndrome. However, note that subclavian steal is observed on 2% of cerebral angiograms and causes no symptoms.
EMBOLISM
Embolism is considered the most common cause of acute arm ischemia (74%). The emboli are attributed to a variety of sources. Cardiac embolism is the most frequently reported cause of acute arm ischemia (58% to 93%) and atrial fibrillation is the usual etiology. Over the years the incidence of atrial fibrillation has remained fairly constant although the cause of fibrillation has changed from valvular heart disease as a result of rheumatic fever to ischemic heart disease and myocardial infarction. Rare causes include endocarditis, atrial myxoma, ventricular aneurysm, cardiac failure, and paradoxical embolism.
Non-cardiac embolism determines 1% to 32% of the acute arm emboli. Proximal upper limb stenosis caused by atherosclerotic plaque or external compression (cervical ribs) can result in thrombo-embolism or atheroembolism, which may cause large vessel occlusion or acute digital ischemia.
Other causes include atheroma in the aortic arch, primary subclavian aneurysm or aneurysm secondary to extrinsic compression from thoracic outlet syndrome, old fracture, and chronic trauma such as that from the use of crutches. Rarer sources are the proximal end of an occluded axillofemoral graft, arteritis, malignant emboli, and fibromuscular dysplasia. Despite a classic embolic presentation and operative findings, an embolic source may not be found in at least 12% of patients.
THROMBOSIS
Reports suggest that 5% of cases in population studies and 9% to 35% in surgical series are due to thrombosi. Jivegard et al. estimated that in patients who had embolectomy, the chance of thrombosis being the true cause was 5.5% in the arm. Most of the proximal arterial lesions that can cause emboli can also result in thrombosis, including atherosclerotic plaques, aneurysm, acute aortic dissection, and arteritis (Takayasu's disease).
Atherosclerosis in the upper extremity appears especially prominent in older men. The disease may be at the origin of the great vessels or distally in the axillary or brachial arteries. Aneurysms of the subclavian or axillary arteries may also result in upper extremity ischemia through two mechanisms. They may directly cause ischemic symptoms by thrombosis or by producing emboli that occlude the distal circulation (Raynaud's phenomenon).
Less common causes include arteritis from connective tissue disorders (scleroderma), radiation arteritis, hyperthrombotic conditions and thrombosis associated with malignancy or steroid use.
|
|
|
|
|
Дата добавления: 2014-12-23; Просмотров: 401; Нарушение авторских прав?; Мы поможем в написании вашей работы!